2 years into the COVID19 pandemic, the fight for vaccine equity continues..
On Thursday last week, I was invited to participate in the Africa-Europe Foundation high-level special dialogue on Addressing the Vaccine Challenge for a renewed Africa-Europe partnership ahead of the 6th Africa-Europe Summit. I was (still am) absolutely honoured to have been able to listen in on such a crucial and important topic with leaders leading the charge on the African continent from WHO, Africa CDC to name a few as well as those from the EU; who are all committed to equitable access to health for all. This debate was very timely and looked at several factors at play in the access to equitable health for all in the context of COVID19 vaccinations. As I listened to the vital points being raised, while it was encouraging to see this conversation occur, it was also bittersweet as personally, it felt like ‘similar challenges, different disease, epidemic, outbreak or now pandemic’.
To provide some context, in 2016, I was selected as European Development Day young leader where I debated on high level panel organised by Politico about achieving sustainable healthcare with the decision makers such as Mark Dybul, then Executive Director of Global Fund, Martin Seychell, then Deputy Director General DG SANTE, European Commission and other highly esteemed leaders. Having deployed to Guinea during the biggest Ebola outbreak in West Africa with the World Health Organisation and the European Mobile Laboratory, I shared my experiences from working on ground. As part of the lessons learnt, we talked about the need for health system strengthening, equal partnerships and local capacity development. I questioned if we as a collective are actually learning the lessons from epidemics and pandemics to ensure we are more proactive rather than reactionary.

Elsa Zekeng, Young Leader, European Development Days 2016, Mark Dybul, then Executive Director, The Global Fund, Ronald de Jong, then Executive Vice-President and Chief Market Leader, Royal Phillips, Martin Seychell, then Deputy Director General DG SANTE, European Commission, Christiaan Rebergen, then Deputy Director for International Cooperation, Ministry of Foreign Affairs, The Netherlands, Martha Rojas-Urrego, then Head of Global Advocacy, Care International, Bob Collymore, then CEO Safaricom, Moderator, Ryan Heath, then Senior EU Correspondent and Associate Editor, POLITICO
During this debate, this sentiment was reverberated by Dr. Matshidiso Moeti – WHO regional Director for Africa as she stated that she was encouraged by this conversation and the investment and pledges being made to reach vaccine equity on the continent. However, she also stated, that as a continent, Africa has gone through several outbreaks and it was not so long ago that these conversations were occurring with regards to HIV/AIDS when patients were unable to access ARVs and positive outcomes emerged. Similarly, after the Ebola outbreak, there was a global movement from a global health security vantage point to establish a response. She stated, all the investment is deeply appreciated but this is a time of crisis, she hopes (I believe this is all of our hope) that we can reach a place where we demonstrate equity, investment and solidarity in times of peace and not just in a pandemic. She continued “We hope that the next crisis will find these investments have been sustained so Africa is found in a better situation and our health systems can contain the impact of an outbreak and continual delivery of services”. Hearing this, I definitely felt comforted but also reminded that achieving equitable partnerships and access to healthcare is truly a marathon and not a sprint considering Dr. Matshidiso Moeti has been in this sector for the better part of 20 years.
As the debate ensued, Pascal Lamy, a trustee from friends of Europe asked thought-provoking questions on if the lack of trust from Africa towards Europe had changed as well as what the status was on the bottle necks that have prevented fair access to vaccines on the African continent. These questions were very welcomed and appreciated by all and vocalised by Dr. Mo Ibrahim as he thanked Pascal for taking this conversation past political correctness and politeness. Dr. Raji Tajudeen – Head of Africa CDC public health institute and research responded to Pascal’s questions highlighting that yes, Africa felt let down as once again we saw nationalism at play, not just in terms of vaccines but also other medical supplies. He provided context to the challenges faced on the African continent stating that “there are 1.2-1.3 billion people in Africa, to get to WHO target of 70% COVID19 vaccine coverage, we need to immunise around 900 million people, through COVAX, we have 350 million vaccines, through the Harvard mechanism we have 400 million vaccines. In terms of supply, we aren’t doing badly. However, what is the point of vaccines if they aren’t getting into people’s arms. The greatest challenge is delivery, last mile delivery on one hand and creating the necessary demand for people to take the shots.” Additionally, he shared that CDC Africa and London School of Hygiene and Tropical Medicine conducted a multinational arm survey in late 2020 which was repeated 3-4 months ago and it showed 4 out of 5 Africans were ready to take these vaccines. Of the 20% who were unsure, it was not necessarily a case of anti-vaxxers but more so the need for more information.

Average acceptance of the COVID-19 vaccine across studies and subgroups within studies. The average acceptance rate across the full set of LMIC studies is 80.3% (95% confidence interval (CI) 74.9–85.6%).
One of the main challenges raised during this debate was the fact that many vaccines arriving on the continent were close to their expiry date making it almost impossible for countries with already limited resources and mechanisms to deploy these fast enough for use. This led to the release of the joint statement from WHO, GAVI, UNICEF, CEPI, African Union, African CDC requesting all vaccines being donated to Africa need to have a minimum of 10 week shelf life when they arrive on the continent among other things. Ashleigh Furlong, a journalist from politico questioned if this had a part to play in vaccine hesitancy as citizens could feel they were getting vaccines ‘Europe doesn’t want”. Dr. Raji Tajudeen commented on this stating that vaccine hesitancy is multifactorial and underpinning this is a lack of adequate information. Dr. Mo Ibrahim echoed these sentiments but also highlighted that hesitancy is a global phenomenon and not an African one as this was evident in Austria, Switzerland, USA and many other countries. It has more to do with us as human beings, misinformation or disinformation. He went on to state that the challenges being faced are not a result of a lack of ‘knowledge on what to do” but rather the angle the political landscape brings. Several pledges were made in 2020 from several world leaders coining the phrase – “nobody is safe until we are all safe”. We all used that phrase, including myself in May 2021 as I wrote about vaccine equity. However, several of these pledges seem to have fallen through the cracks as we continue this conversation 2 years on.
European Commissioner for International partnerships, Ms Jutta Urpilainen responded admitting that yes there is a still a lot to be done but also defended the EU politicians stating that in terms of donations and financial support, the EU has led the efforts within the international community to assist African countries to attain vaccine equity. This solidarity led to founding COVAX and so far, 1.45 billion vaccines have been exported to Africa. She continued highlighting that out of €46 billion contributed to help 146 countries cope with the pandemic, €10 billion has gone to Africa. She stated that the EU has committed to share at least 700 million doses by mid 2022, about half of the vaccines donated has reached Africa. However, we know donating vaccines is just one part of the challenge while ensuring they make it to people’s arms is the other. She emphasised that in the short term, the EU will continue to support the urgent response to COVID19 including vaccine deployment as €100 million has been contributed to support vaccine deployment in Africa. This will have a dedicated vaccine support package to roll out at country level.
Dr. Mo Ibrahim returned the accountability to Africa stating that Africans have made mistakes, the health systems are weak and so is data collection and countries need to strengthen their Office for National Statistics. When we review the Abuja declaration, the spend agreed on the health sector was 15% of their annual budget, however, countries average between 6-8% spend. This has improved over the years but is still not in accordance with what was agreed in many years ago. Therefore, African countries have a lot of adjustments to make in-country before blaming anyone else.
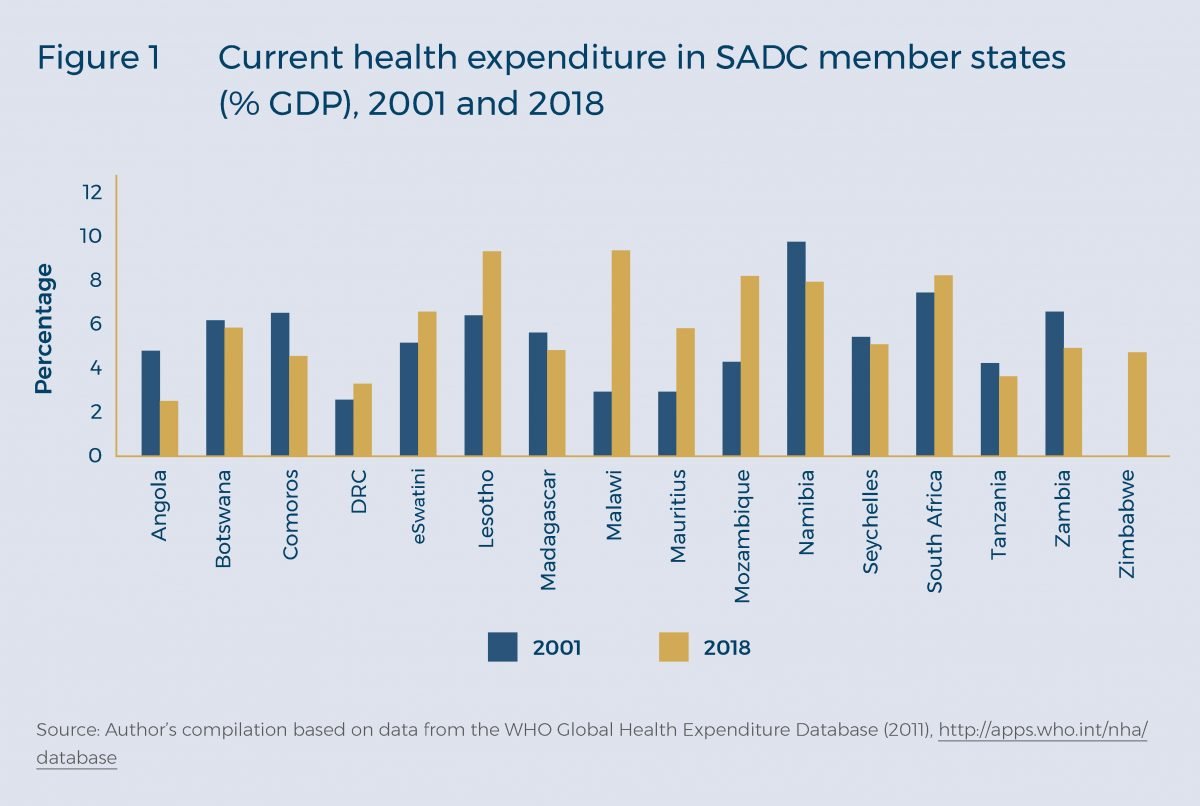
A snapshot of health expenditure from countries in the Southern African Development Community (SADC)
As the AU-EU partnership seeks sustainable solutions to arrive vaccine equity, a critical component is development of vaccines on the African continent to allow for capacity building and quicker vaccine deployment. Dr. Marie-Paule Kieny highlighted the importance of local production of vaccines on the African continent owned by African government with technology free of rights to produce not only COVID vaccines but HIV, TB and any other infectious diseases. She stated that Afrigen in South Africa will develop the technology and transfer this to multiple partners (to be announced by Dr. Tedros Adhanom, Director General of the World Health Organisation). Dr. Morena Makhoana, CEO of Biovac highlighted the importance of the private sector as a stakeholder, the importance of looking at Africa as an equal partner, the need to have a market that is sustainable to keep Africa alive and this requires sustained investment accompanied by the right technologies and capabilities. This was supported by input from Dr. Sierk Poetting, COO of BioNTech stating their support to Senegal, Rwanda and South Africa for the construction of decentralised end to end manufacturing network and building local capacity for mRNA through transfer of knowledge. All these points were supported by Martin Seychell, Deputy Director General at DG International Partnerships - European Commission, stating that the business case for Africa to have a vaccine development hub is clear but we need to ensure that the support from partners is leveraged, human resource is built, the ecosystem is de-risked to encourage further investment and pharmaceutical research is supported, as it is from research that entrepreneurship flows.
This debate was moderated ever so gracefully and efficiently by Tamsin Rose, senior fellow for health at the Africa-Europe foundation who finalised the take home messages in the following points; the need for sustained investment, investment in workforce capacity building, building research universities capacity and partnership distribution and clarifying the Africa – Europe direction. In closing, Chrysoula Zacharopoulou, a member of the European parliament and gynaecologist stated that we need to invest in Africa, firstly through the 15% of public finance that was pledged by African Heads of states in the Abuja declaration. Additionally, implementing manufacturing, regulations and mechanisms in partnership with the international community is equally important. However, pushing back on Dr. Mo Ibrahim’s stance on vaccine hesitancy, she stated that in her experience vaccine hesitancy is cultural and trickled into belief systems. She stated that in this renewed partnership, Africa has a role to play in taking care of its citizens and Europe can accompany and support.

This debate was clearly one that is timely and essential to encourage and sustain equal EU-AU partnerships. However, these conversations occur after a crisis as Dr. Matshidiso Moeti stated and we hope these investments are sustained to meet the next crisis. As we continue these conversations for renewed AU-EU partnerships, it is essential that the youth are brought in to participate to understand the historical context of these exchanges following outbreaks from HIV/AIDS to Ebola and now COVID19. Participation that isn’t limited to one event but rather ensuring continuity so that there is increased awareness, preparedness and continued partnership building. In the last 7 years, I have participated in the response to the Ebola outbreak in West Africa and in discussions around changes to be implemented. During this time, I also completed my PhD in Infectious Diseases and Global Health and have keenly followed the COVID19 outbreak; from the science and research, to public perception and attempting to understand human behaviour in unprecedented situations and of course the response from pharmaceutical companies and the interplay between politics and public health. While my eagerness and somewhat frustration makes me think we have had many of these conversations before and noted the lessons learnt, I have to acknowledge that there has been progress but there is more we could have done and can do. I recognise the time and effort it takes to move the needle towards implementing sustained change in our health systems and renew partnerships. This led me to the thought that there needs to be a continuous intergenerational ‘passing of the baton’ and involvement of youth at every stage to provide an understanding and context on what has been done and what still needs to be done. Additionally, investing in ecosystems that are fast growing for example biotech start-up ecosystems in Africa is imperative. The benefits of start-ups include their agility and ability to be more iterative to arrive at quicker solutions in the face of unprecedented situations. Finally, in the short term, these partnerships should include engaging with new partners in the private sector who have the technical knowledge and logistical bandwidth to support in addressing some of these bottlenecks.